
MICRONEEDLING, TYPES, AND EFFECTS
Microneedling: Advances and widening horizons
Abstract
Microneedling is a very simple, safe, effective, and minimally invasive therapeutic technique. It was initially introduced for skin rejuvenation, however, now it is being used for a very wide range of indications including acne scar, acne, post-traumatic/burn scar, alopecia, skin rejuvenation, drug delivery, hyperhidrosis, stretch marks, and many more. Moreover, during the last 10 years, many new innovations have been made to the initial instrument, which was used for microneedling. This technique can be combined with other surgical techniques to provide better results. In particular, it is a very safe technique for dark skin types, where risk of postinflammatory pigmentation is very high with other techniques that damage the epidermis. In this review article, we are updating on the different instruments now available for this procedure, and its efficacy when performed alone or in combination with other techniques for various indications.
Keywords: Dermaroller, dermatosurgery, microneedling, percutaneous collagen induction
INTRODUCTION
Microneedling is a relatively new minimally invasive procedure involving superficial and controlled puncturing of the skin by rolling with miniature fine needles. Over a short period of time, it has gained mass popularity and acceptance as it is a simple, cheap, safe, and effective technique requiring minimal training. Traditionally used as a collagen induction therapy for facial scars and skin rejuvenation, it is also widely used now as a transdermal delivery system for therapeutic drugs and vaccines. In this review, we highlight the constantly evolving research and developments in microneedling techniques, instruments, and its applications in dermatology.
Microneedling is a relatively new minimally invasive procedure involving superficial and controlled puncturing of the skin by rolling with miniature fine needles. Over a short period of time, it has gained mass popularity and acceptance as it is a simple, cheap, safe, and effective technique requiring minimal training. Traditionally used as a collagen induction therapy for facial scars and skin rejuvenation, it is also widely used now as a transdermal delivery system for therapeutic drugs and vaccines. In this review, we highlight the constantly evolving research and developments in microneedling techniques, instruments, and its applications in dermatology.
THE INVENTION
The advent of the concept of microneedling dates back to 1995 when Orentreich and Orentreich described dermal needling in the form of subcision for scar treatment and then independently in 1997 by a plastic surgeon Camirand who used tattoo guns without ink to take-off tension from postsurgical scars.[1,2] Microneedling technique was given further shape by a German inventor Liebl in 2000 and a plastic surgeon Fernandes in 2006 who self-designed a drum-shaped device with multiple fine protruding needles and used it for percutaneous collagen induction.[3,4]
BASIC INSTRUMENT
The standard medical dermaroller [Figure 1] has a 12 cm long handle with a 2 × 2 cm wide drum-shaped cylinder at one end studded with 8 rows and 24 circular arrays of 192 fine microneedles, usually 0.5–3 mm in length and 0.1–0.25 mm in diameter.[3] These single use microneedles are synthesized by reactive ion etching techniques on silicon or medical-grade stainless steel. The instrument is presterilized by gamma irradiation. Rolling with a standard dermaroller containing 192 needles of 2 mm length and 0.07 mm diameter over an area of skin for 15 times results in approximately 250 holes per square cm upto the papillary dermis depending on the pressure applied.[5] Each pass produces 16 micropunctures in the stratum corneum per square cm without damaging the epidermis significantly.[6]
Principle and mechanism of action
Micropunctures are created using microneedles which produce a controlled skin injury without actually damaging the epidermis. These microinjuries lead to minimal superficial bleeding and set up a wound healing cascade with release of various growth factors such as platelet derived growth factor (PGF), transforming growth factor alpha and beta (TGF-α and TGF-β), connective tissue activating protein, connective tissue growth factor, and fibroblast growth factor (FGF).[7] The needles also breakdown the old hardened scar strands and allow it to revascularize. Neovascularization and neocollagenesis is initiated by migration and proliferation of fibroblasts and laying down of intercellular matrix.[8,9] A fibronectin matrix forms after 5 days of injury that determines the deposition of collagen resulting in skin tightening persisting for 5–7 years in the form of collagen III. The depth of neocollagenesis has been found to be 5–600 µm with a 1.5 mm length needle. Histological examination of the skin treated with 4 microneedling sessions 1 month apart shows upto 400% increase in collagen and elastin deposition at 6 months postoperatively, with a thickened stratum spinosum and normal rete ridges at 1 year postoperatively.[10] Collagen fibre bundles appear to have a normal lattice pattern rather than parallel bundles as in scar tissue.[6]
Liebl et al. have proposed another hypothesis to explain how microneedling works.[11] Resting electrical membrane potential of cells is approximately −70 mV, and when needles come near the membrane, the inner electrical potential increases quickly to −100 mV. This triggers increased cell activity and the release of various proteins, potassium, and growth factors from the cells into the exterior leading to the migration of fibroblasts to the site of injury, and hence, collagen induction. Thus, the needles do not create a wound in a real sense, but rather body cells are fooled into believing that the injury has occurred.[9,11,12,13]
The expression of matrix metalloproteinases induced by microneedling is speculated in reduction of hyperpigmentation.[11] In addition, the hyperproliferation of keratinocytes is downregulated by microneedling in acne patients because it overall balances out the cell equilibrium.[11] However, more research needs to be done to elucidate the chain of events clearly.
Microneedling enhances the delivery of various drugs across the skin barrier as it bypasses the stratum corneum and deposits the drug directly up to the vascularized dermis. It has also been shown to cause significant widening of the follicular infundibulum by 47%, which may partly explain the increased penetration of the medication across the skin barrier. In addition, it removes the scales and sebum residues in the neighbourhood of the infundibulum.[14]
Hence, this procedure extrapolates the body’s own physiology of wound healing and the new collagen deposition results in skin tightening and filling-up of atrophic scars with an overall better aesthetic appeal since overlying epidermis is not ablated.
PROCEDURE
Microneedling is a simple office-based procedure lasting 10 to 20 minutes depending on the area to be treated. The patients must be counselled prior to the procedure explaining the expected outcomes, delayed response, and need for multiple sittings. The skin should preferably be prepared preoperatively for at least a month with vitamin A and C formulations twice a day to maximize dermal collagen formation. Vitamin A influences 400–1000 genes that control proliferation and differentiation of all major cells in epidermis and dermis, and Vitamin C is essential for production of normal collagen.[10]
The procedure is performed under topical anesthesia containing eutectic mixture of lignocaine and prilocaine/tetracaine for 45 minutes to 1 hour. After preparation of the area with antiseptic and saline, the skin is stretched with one hand, and perpendicularly, rolling is done 5 times each in the horizontal, vertical, and oblique directions with the other hand [Figure 2]. The treatment endpoint is identified as uniform pin-point bleeding which is easily controllable. Post-procedure, the area is made wet with saline, or ice packs can be used for comforting the patient. Thereafter, the patient is advised to use sunscreen regularly and follow sun-protective measures. The procedure is well-tolerated by the patients and there are usually no post-treatment sequelae except slight erythema and edema lasting for 2–3 days. There is no downtime and the patient can resume daily work the very next day. Treatments are performed at 3–8 week intervals and multiple sittings are needed to achieve the desired effect on the skin. The final results cannot be viewed immediately because new collagen continues to be laid down for approximately 3–6 months after treatment has ceased.[10,15]

VARIOUS INSTRUMENTS AND TECHNIQUES
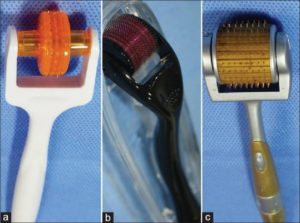
A simple dermaroller has evolved over the past decade through a variety of advancements. The current market is booming with an assortment of devices based on needle length, drum size, and automation [Figure 1].
The most important is the diversity of needle lengths. High ratio of tip length versus diameter of 13:1 is an important property of good needles.[6] The length of needle selected for an individual patient depends upon the indication for microneedling. For treating acne and other scars as a routine, a needle length of 1.5–2 mm is usually used. When microneedling is used as a procedure to treat ageing skin and wrinkles, the needle length of 0.5 mm or 1.0 mm is usually recommended.[9] When the needles are only up to 0.5 mm long, the procedure is essentially painless, and the perception of pain increases as the depth of needle penetration increases. It also depends on the thickness of epidermis and dermis of the skin.
The minimum time interval between two sittings of microneedling depends upon the indication for which the procedure is being done as well as the needle length of the dermaroller being used. More is the needle length, greater should be the interval between two sittings of microneedling. When using 1.5 mm dermaroller, at least 3 weeks gap should be there between two procedures.
Five basic types of medical dermarollers, which are registered with the FDA, have been described in the dermaroller series by Konstantinos, and most dermarolling devices are adopted from these elementary types:[16]
-
C-8 (Cosmetic type), is the basic dermaroller as described above with a needle length of only 0.13 mm (130 μm) used for enhancing penetration of topical agents. It is completely painless.
-
C-8HE (Cosmetic type for hair-bearing surfaces, scalp) has a needle length of 0.2 mm (200 μm). Even this length is below the pain threshold.
-
CIT-8 (CIT: Collagen Induction Therapy, Medical type) has a needle length of 0.5 mm (500 μm) and helps in collagen induction and skin remodelling.
-
MF-8 type has a needle length of 1.5 mm (1500 μm). This creates deeper microchannels on the whole epidermis and dermis and at the same time destroys scar collagen bundles.
-
MS-4 is the only dermaroller that has a smaller cylinder, 1 cm length, 2 cm diameter, and subsequently 4 circular arrays of needles (total 96 needles) that have 1.5 mm length. It is used on areas where better precision and deeper penetration is required. It is mostly used on facial acne scars.
-
Devices similar to MS-4 are available with needle lengths of 0.5–0.75 mm, which are used for thin-skinned areas such as the periorbital and perioral regions.
Home care dermaroller
Home-care dermarollers (C-8) are used by patients themselves as they are of needle length less than 0.15 mm and are available for reduction of pore size, fine lines, and sebum production, as well as for transdermal delivery of substances such as lipopeptides and other antiageing products. They can be used twice or thrice a week for up to 100 times. After use, the rollers should be cleaned in hot tap water and shaken dry.[3,17] Beauty Mouse is another approved device intended for home use. It contains a total of 480 needles of approximately 0.2 mm size on 3 separate drums strategically placed inside a computer mouse shaped device. It has been developed to ensure coverage of larger skin surface areas, such as the arms, legs, and buttocks for the treatment of stomach or thigh stretch marks and cellulite.[18]
Derma-stamp
These are miniature versions of the dermaroller available in different needle lengths (0.2–3 mm) and a diameter of 0.12 mm that are used for localized scars such as varicella scars. Advantage over the dermaroller is that a more focussed treatment of individual scars is possible. It causes vertical penetration to create infusion channels in the skin and is considered ideal for use on isolated scars and wrinkles.[3,5,17,18]
Dermapen
Dermapen [Figure 3] is an automated microneedling device which looks like a pen. This ergonomic device makes use of disposable needles and guides to adjust needle length for fractional mechanical resurfacing. The tip has 9–12 needles arranged in rows. It makes use of a rechargeable battery to operate in two modes, namely, the high speed mode (700 cycles/min) and the low speed mode (412 cycles/min) in a vibrating stamp-like manner.[19] It has the advantage of being reusable in different patients as the needles are disposable, safe as the needle tips are hidden inside the guide, and more convenient to treat narrow areas such as the nose, around the eyes and lips without damaging the adjoining skin. It makes the procedure less painful and more economical as there is no need to buy a new instrument every time.[20] This technology has been designed to overcome the issues of varying pressure application and the subsequent depth of penetration achieved.[18]

Dermapen with battery charger
DermaFrac
DermaFrac treatment is a newer modification of microneedling combining microdermabrasion, microneedling, simultaneous deep tissue serum infusion, and light emitting diode (LED) therapy. DermaFrac treatments target aging and sun damaged skin, acne, enlarged pores, uneven skin tone, wrinkles, fine lines, hyperpigmentation, and superficial scars. It takes approximately 45 min to complete full face treatment when all four modalities are used. This noninvasive, cost-effective treatment carries the advantage of having no downtime with individualized selection of serums for infusion.[20,21]
Microneedle delivery systems
Microneedle delivery systems offer a minimally invasive and painless method of transdermal drug administration, especially useful for vaccines.[22] The various types of microneedles available for this purpose can be solid, coated, dissolving, hollow, and swellable polymer microneedles synthesized by microfabrication technique.[18] Silicon, metals such as titanium, natural and synthetic polymers, and polysaccharides are the various materials used to fabricate these microneedles. Solid-coated microneedles are used to pierce the superficial skin followed by topical application and delivery of the drug, whereas dissolvable or biodegradable and hollow needles deliver drugs directly into the dermis.[22]
Fractional radiofrequency microneedling
The amalgamation of microneedling with radiofrequency has further expanded the prospects of application of this technology. Insulated needles are used to penetrate the skin and release radiofrequency currents from the needle tips producing thermal zones in the dermal structural components and accessory glands without damaging the overlying epidermis.[23] This triggers long-term dermal remodelling, neoelastogenesis, and neocollagenesis. The depth of the needles can be adjusted from 0.5 mm to 3.5 mm allowing us to target different layers of the dermis discretely.[24] Operating person can exercise a good control over tissue damage by adjusting the power level and duration of energy pulse. The main energy delivery system has a disposable tip with 49 gold plated needles. Microneedling radiofrequency (MNRF) technology does not damage the epidermis, and is therefore, safe in darker skin types. Its indications include scar treatment, hyperhidrosis, skin tightening, rejuvenation, and many more.
Light emitting microneedling device
LED microneedling rollers have been recently launched. These incorporate titanium microneedles and LED light to combat wrinkles and scarring.[19] These devices have not yet been explored and no published data is available regarding its efficacy.
APPLICATIONS OF MICRONEEDLING IN DERMATOLOGY
Dermarolling has been used for a wide range of indications with many trials supporting evidence for its usefulness.[5,6,17,23] It has been tried alone as well as in combination with other treatment modalities such as chemical peeling, platelet rich plasma, radiofrequency, subcision, punch elevation, and lasers. It is often used in conjunction with a topical formulation, and hence, enhances its penetration and action.
Skin rejuvenation
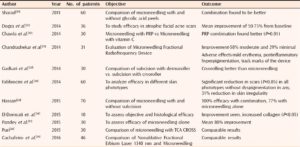
Microneedling leads to reorganization of old collagen fibres and laying down of new collagen, elastin, and capillaries leading to the effect of skin tightening. A significant increase in level of collagen type I, III, and VII, newly synthesized collagen and tropoelastin from baseline was observed after 6 microneedling sessions at 2-week intervals by El-Domyati et al.[25] This percutaneous collagen induction leads to an overall youthful appearance of the skin by reducing fine lines and wrinkles, reducing pore size, more suppleness, and elasticity.
The effects are enhanced when the procedure is combined with topical antiageing vitamin C serum and tretinoin application. Microneedling has also been combined with human embryonic stem cells derived endothelial precursor cell conditioned medium and has shown significant reduction in wrinkles and pigmentation.[26,29] Fractional microneedling radiofrequency has been studied in a large multicentre trial and has found to be effective in reducing wrinkles [Table 1].[27]

Scars
Acne scars
The most frequently used indication of microneedling is post-acne facial atrophic scars [Figure 4], and a large number of trials have been conducted to evaluate the same alone as well as in combination with chemical peels, platelet-rich plasma, subcision, cryotherapy, and CROSS technique. Microneedling has been found to be more effective for rolling and boxcar scars, and relatively less effective in ice-pick scars. It is safe for all skin types with minimal downtime. Only the affected area needs to be treated and there is minimal risk of post-inflammatory dyschromia. However, a minimum of 4–6 sessions are required for a significant improvement [Table 2].

Pre (a, c, e) and post (b, d, f) treatment photographs of post-acne atrophic scar patients after 4 sittings of microneedling done 1 month apart
Table 2
Studies using miconeedling for facial post acne atrophic scars (literature search after year 2010)
Nonacne scars
Post-burn scar, post-traumatic scar, hypertrophic scars, varicella scars [Table 3].
Table 3
Microneedling for non-acne scar treatment (literature search after year 2010)

Post-surgical scars were the first to be studied by Camirand[2] who used tattoo gun needles to reduce the scars. Since then, microneedling has been used for almost all types of surgical scars and are to be found useful. Microneedling has been found to be effective in reducing even burn scars [Figure 5] by up to 80% in a study on 16 patients by Aust et al. It was stipulated that there is normalization of collagen-elastin matrix in the dermis at 1 year.[10,15] Microneedling is also effective for varicella scars [Figure 6] and post-traumatic scars [Figure 7].

Post-burn scar on the thigh of 1 year duration treated with a combination of microneedling and laser (a) Baseline photograph; (b). Scar showing improvement after 3 fortnightly sessions of microneedling; (c) Further improvement in scar following 1 session of Fraxel laser RE: STORE SR 1500nm (Solta Medical, USA) with following parameters: 70 mj beam energy, 20% density, 8 passes. (Courtesy: Dr Arshdeep, Consultant Dermatologist, Kubba Skin Clinic, New Delhi)

Post-varicella scars (a,c) showing improvement (b,d) after 3 microneedling sittings done 1 month apart

Significant improvement in post-traumatic scar over the nose after 1 sitting of subcision followed by 3 sittings of microneedling done 1 month apart
Acne vulgaris
The advent of fractional microneedling radiofrequency has expanded the application of microneedling to acne vulgaris as well. It directly targets the sebaceous glands and helps in reducing the sebum production. It is also known to reduce the hyperproliferation of keratinocytes [Table 4].

Androgenic alopecia and alopecia areata
Use of microneedling over scalp for alopecia is one of its recent advances. It has been compared with minoxidil alone and has been found to be better in combination.[47,48] Home-use dermarollers are prescribed to patients who are using minoxidil, and a better hair growth is observed. However, when topical minoxidil was compared with Platelet Rich Plasma (PRP) and microneedling therapy in a recent study, minoxidil alone continued to remain better.[49] Microneedling has also been combined with topical triamcinolone acetonide application in alopecia areata and better response has been observed [Table 5].[50]
Table 5
Microneedling trials for alopecia (literature search after year 2010)

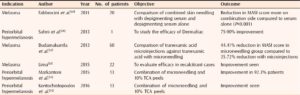
Pigmentation—Melasma and periorbital hypermelanosis
The introduction of Dermafrac technique and smaller drums with needles sizes approximately 0.5 mm has made the microneedling to periocular skin amenable. Microneedling has been combined with various skin lightening agents and chemical peels to reduce melasma as well as periorbital hypermelanosis [Table 6].
Table 6
Microneedling trials for pigmentation (melasma and periorbital hypermelanosis) (literature search after year 2010)
Miscellaneous conditions
Extended applications of microneedling include stretch marks, axillary hyperhidrosis, and actinic keratosis in photodamaged skin. MNRF has been used even in patients with rosacea and post-acne erythema with favorable results [Table 7].
Table 7
Microneedling trials for miscellaneous indications (literature search after year 2010)

TRANSDERMAL DELIVERY OF DRUGS
The technique of microneedling has been well-exploited to increase penetration of drugs across the skin barrier. This has been proven in in-vitro skin models where enhanced absorption of larger molecules such as calcein has been observed.[62,63] Microneedles cover a range of activity between that of a transdermal patch and a hypodermic needle attempting to gain the advantages of both and eliminate the disadvantages of each one of them. Microneedling has been used for the transdermal delivery of various types of drugs including macromolecular biopharmaceuticals such as insulin, growth hormone, heparin, and albumin; immunobiologicals such as hepatitis B, tetanus toxoid, and influenza vaccines; proteins, peptides and drugs such as aspirin, minoxidil, tretinoin, and L-ascorbic acid.[21,64,65] Microneedling has also been combined with other advanced techniques such as micropumps, sonophoresis, iontophoresis, and electroporation for better drug penetration.[21]
With respect to dermatology, microneedling is often combined with topical tretinoin and vitamin C for the treatment of acne scarring and skin rejuvenation, as described above. Penetration enhancement of minoxidil and platelet-rich plasma for androgenic alopecia is another application. Microneedling enhances the effect of 5-aminolevulinic acid for more efficacious photodynamic therapy.[66] They have been used in combination for the treatment of actinic keratosis[56] and photoaging.[28]
CONTRAINDICATIONS[5,6]
-
Active acne
-
Herpes labialis or any other local infection such as warts
-
Moderate to severe chronic skin disease such as eczema and psoriasis
-
Blood dyscrasias, patients on anticoagulant therapy
-
Extreme keloidal tendency
- Patient on chemo/radiotherapy.
LIMITATIONS AND ADVERSE EFFECTS
Dermarolling has its own set of limitations despite its assembly of effective uses and advantages over other procedures. It is less efficacious in some types of scars such as pitted scars, linear scars, and deep boxcar scars. However, combining other surgical procedures to microneedling can improve its results.
Certain adverse events are also known with the procedure, the common ones being potential erythema and irritation which usually subside within a few hours. Other events noted are post-inflammatory hyperpigmentation, aggravation of acne and reactivation of herpes, systemic hypersensitivity, allergic granulomatous reactions and local infections following the use of a nonsterile instrument.[6,9,17,22] Allergic contact dermatitis to materials used in the needles has also been observed.[67] Tram-track effect after two sessions of microneedling has been reported in a patient with acne scars who developed regularly placed linear papular scars over bony prominences of the face.[68] This can be avoided by using less pressure and smaller needles over these areas.
Microneedling is relatively safe to use in Indian skin because it rarely leads to hyperpigmentation unlike other ablative and resurfacing procedures.[23] It carries a better safety profile with regards to risk of dyspigmentation in all skin types.[34]
FUTURE PROSPECTS
Because skin is an easily accessible tissue, has a good regenerative capacity, and is easily scrutinized directly, it serves as a potential organ for the development of therapeutic and prophylactic genetic medicines. It was demonstrated by Chabri et al. that microneedling can be used for intradermal delivery of a nonviral vector which can be exploited for localized treatment of genetic diseases such as epidermolysis bullosa.[69]
Dermarolling may be useful to dye poorly pigmented hairs and improving laser hair removal because it has been shown that it dilates the follicular infundibulum and increases the transfollicular absorption of melanin.[14]
CONCLUSION
Microneedling is an effective modality of treatment, especially in patients with Fitzpatrick’s IV and V skin types because it overcomes the side effects of scarring and hyperpigmentation resulting from other procedures in which the epidermis is compromised. It certainly promises to be a valuable technique with its numerous applications and its ever-expanding modifications as well as feasibility of home use.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
69. Chabri F, Bouris K, Jones T, Barrow D, Hann A, Allender C, et al. Microfabricated silicon microneedles for nonviral cutaneous gene delivery. Br J Dermatol. 2004;150:869–77. [PubMed]
Articles from Indian Dermatology Online Journal are provided here courtesy of Wolters Kluwer — Medknow Publications
